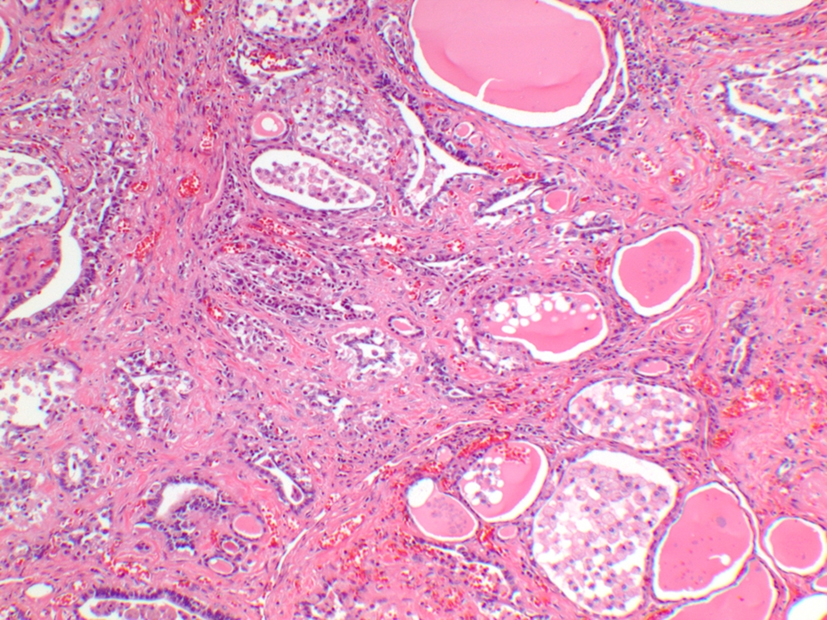
Figure 1. Thyroid gland histopathology demonstrates intra-follicular histiocytes, patchy fibrosis and involuted follicles.
| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website http://www.jofem.org |
Case Report
Volume 5, Number 3, June 2015, pages 220-223
Mixed Amiodarone-Induced Thyrotoxicosis Refractory to Medical Therapy and Plasmapheresis
Figure
Tables
| Hormonal investigations | On presentation | After 8 cycles of plasmapheresis | 24 h post-surgery | 72 h post-surgery | Reference range |
|---|---|---|---|---|---|
| TSH (μIU/mL) | 0.02 | 0.04 | 0.08 | Not tested | 0.28 - 3.89 |
| Free T4 (ng/dL) | 4.88 | 4.54 | 3.25 | 1.72 | 0.58 - 1.64 |
| Free T3 (pg/mL) | 5.4 | 5.3 | 3.7 | 61 | 2.5 - 3.9 |
| Total T3 (ng/dL) | 114 | 111 | 67 | 2.1 | 87 - 178 |
| Features of AIT | Type 1 AIT | Type 2 AIT | Mixed AIT |
|---|---|---|---|
| Mechanism | Excess thyroid hormone synthesis | Excess release of T3, T4 (destructive thyroiditis) | Features of both |
| Predisposed thyroid gland | Abnormal | Apparently normal or small goiter | Features of both |
| I-123 uptake scan | Most commonly low or low-normal, but sometimes normal or increased | Usually very low | Features of both |
| Thyroid ultrasound | Hyper-vascularity | Absent or decreased vascularity | Features of both |
| Management | Thionamides Rare need to add potassium perchlorate (not FDA approved) | Anti-inflammatory therapy like prednisone | Combination of both |