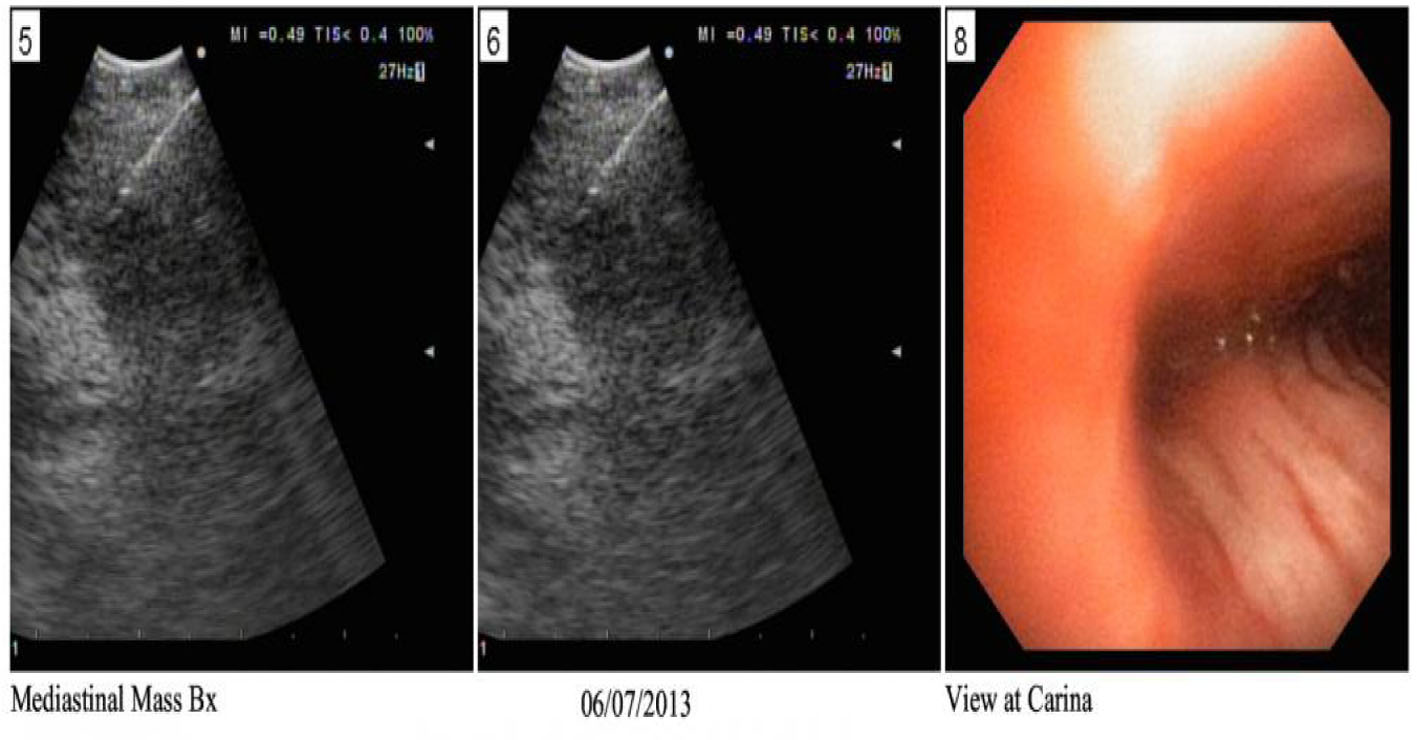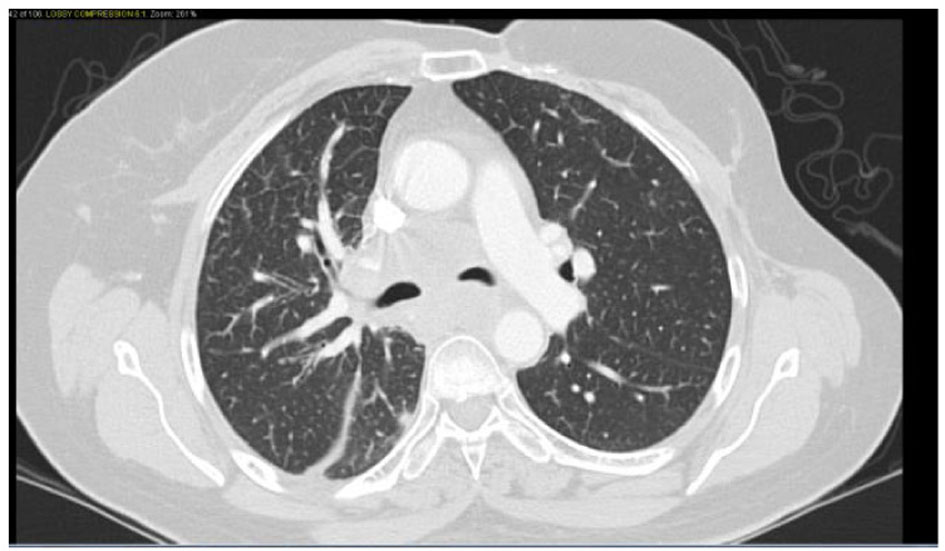
Figure 1. Confluent mediastinal and right hilar adenopathy, likely represent metastatic disease. Peribronchovascular infiltrates in the right lower lobe.
| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website http://www.jofem.org |
Case Report
Volume 5, Number 4, August 2015, pages 256-260
Pituitary Metastasis From Breast Cancer Presenting as SIADH
Figures