Figures
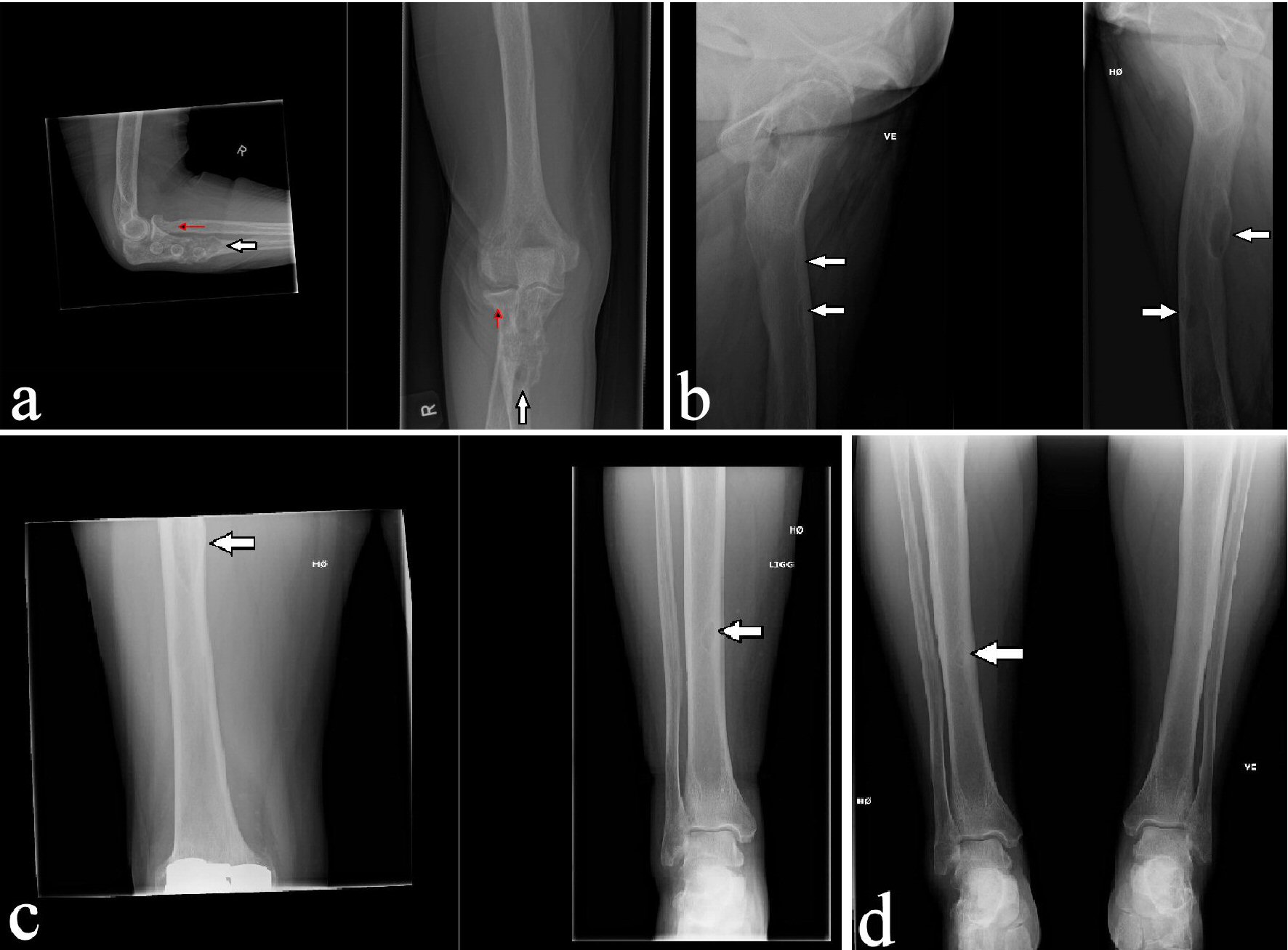
Figure 1. Initial X-ray of the right elbow showing fracture of the head of the radius (red arrow) and an expansive osteolytic lesion in the ulna mimicking sequels after pathological fracture (a) and X-rays of both lower extremities showing osteolytic lesions in both femurs (b) and right tibia (c and d) (white arrows).
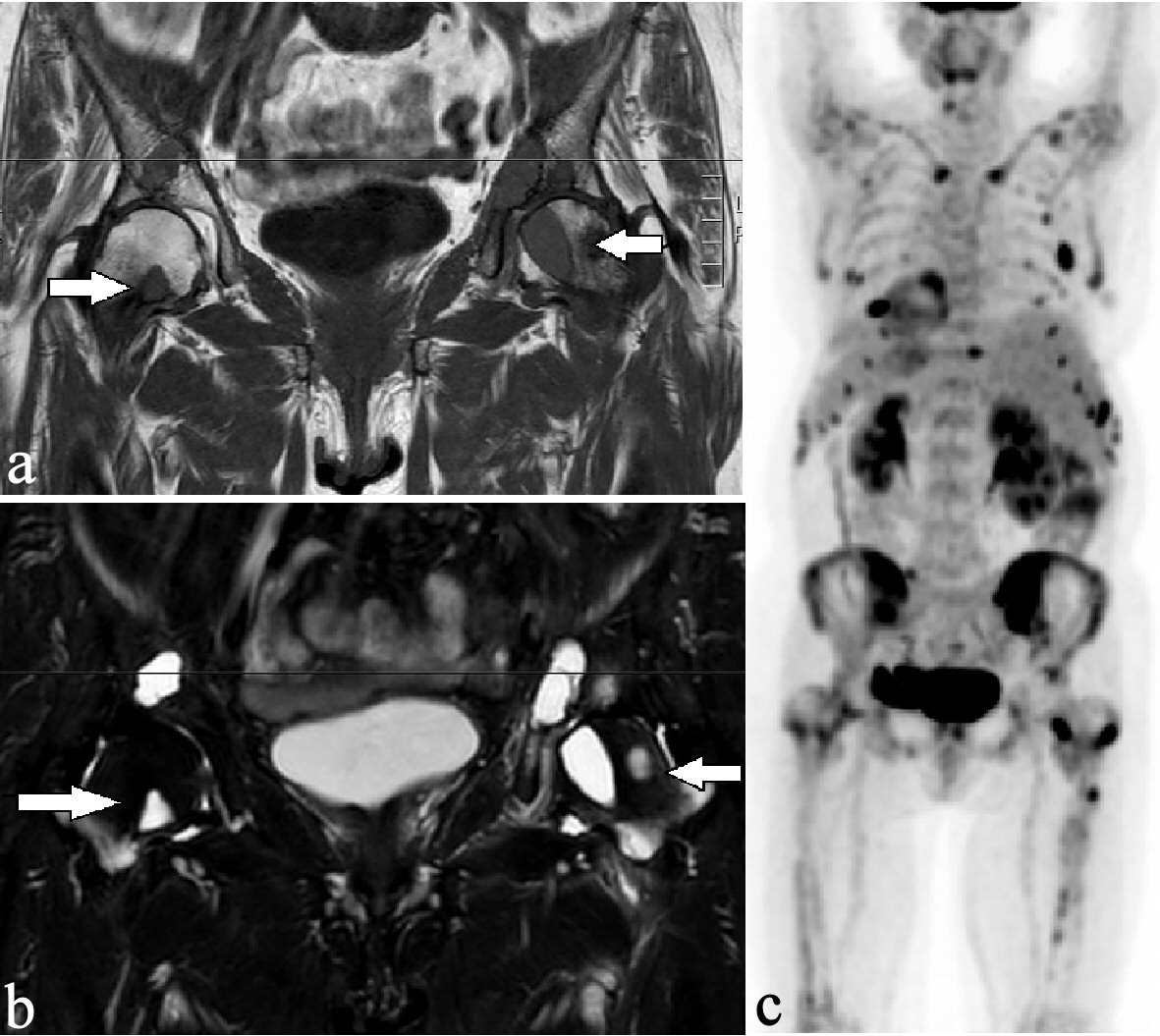
Figure 2. Osteolytic lesions had a low-intensity signal on the T1-weighted sequence (a) and had a high-intensity signal on the STIR sequence (b) in both femurs (arrows). The coronal PET scan showed high (18F) FDG metabolism in multiple osteolytic lesions in the cervical spine, both clavicles, the ribs, the pelvis, and both femurs (c). PET: positron emission tomography.
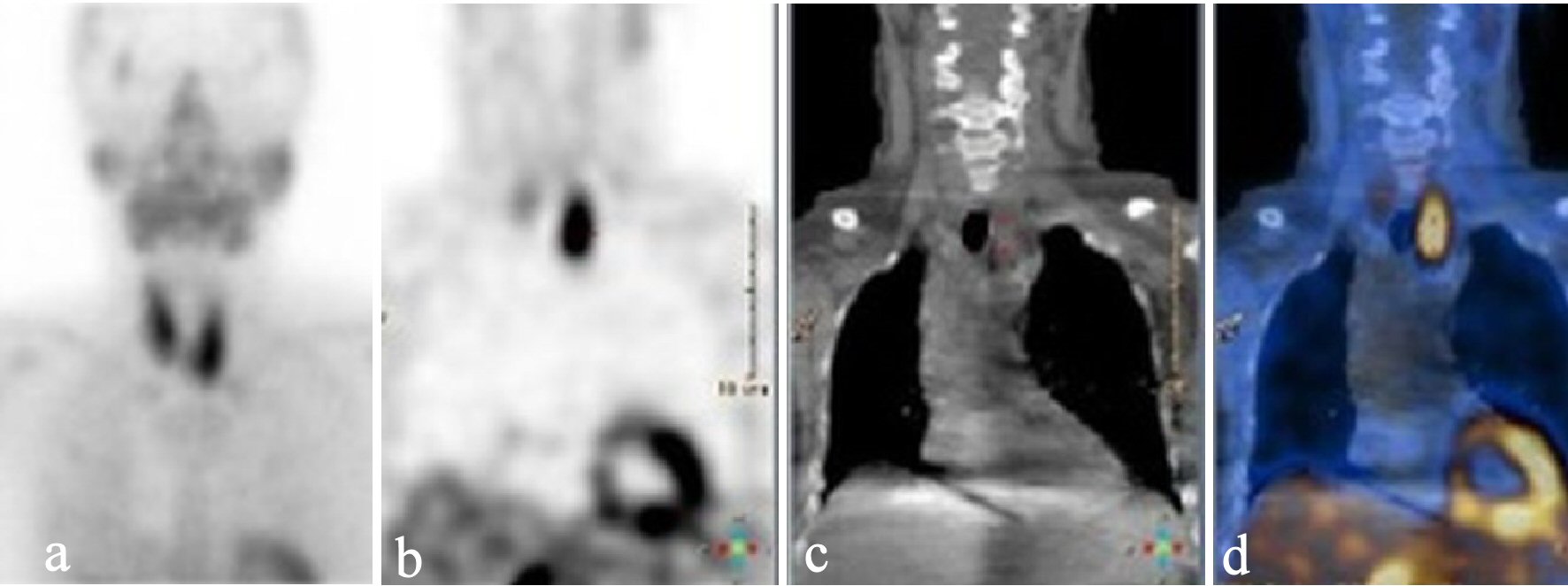
Figure 3. Static parathyroid scintigraphy after injection of 99mTc-pertechnetate in early phase (a), and late phase (after wash-out) (b) showing accumulation related to the caudal part of the left thyroid lobe. Low-dose CT (c) and fused image of the scintigraphy and the low-dose CT (d) suggested a parathyroid adenoma. CT: computed tomography.
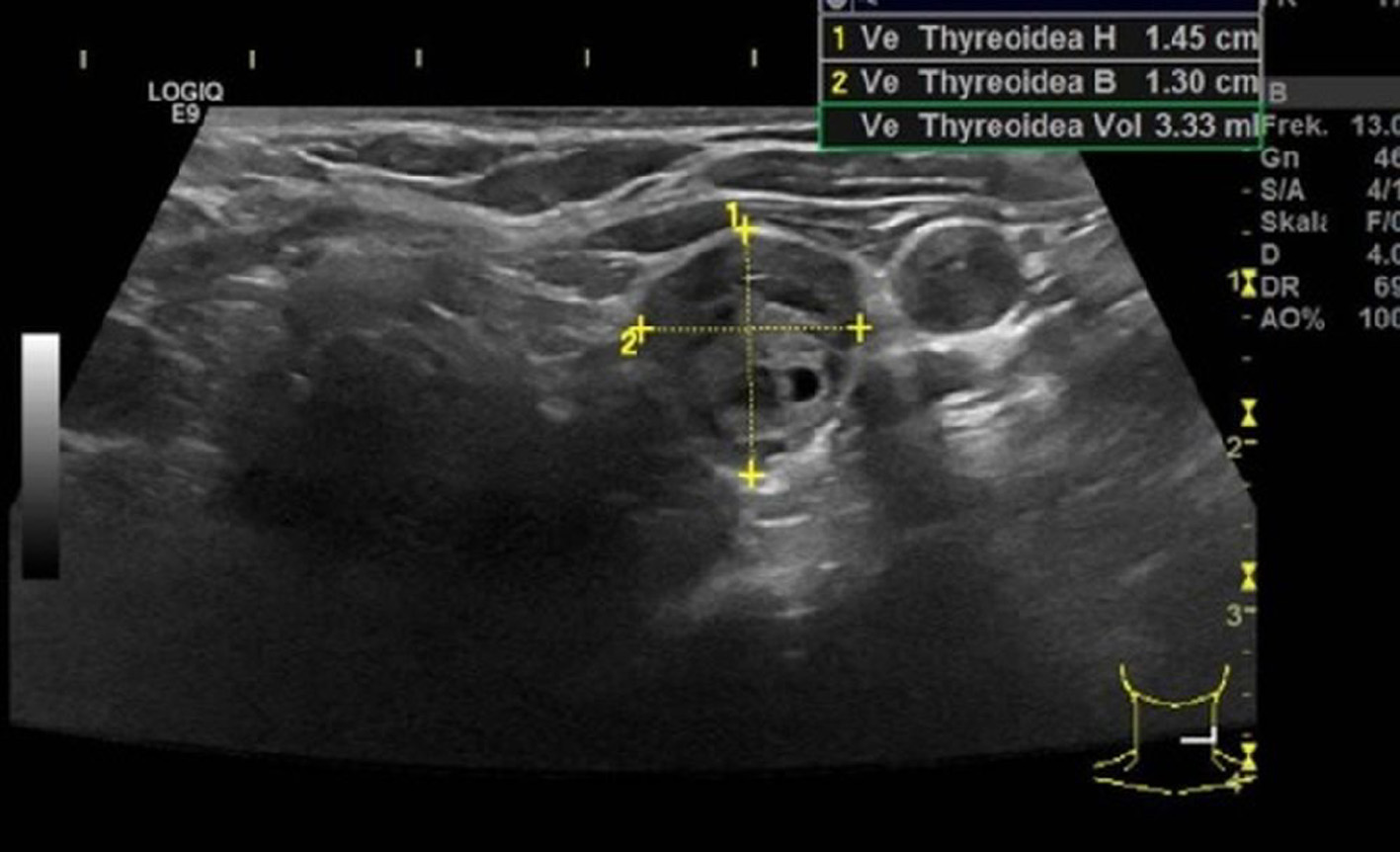
Figure 4. Ultrasound examination showing a hypoechoic adenoma that had an estimated weight of 3.3 g.
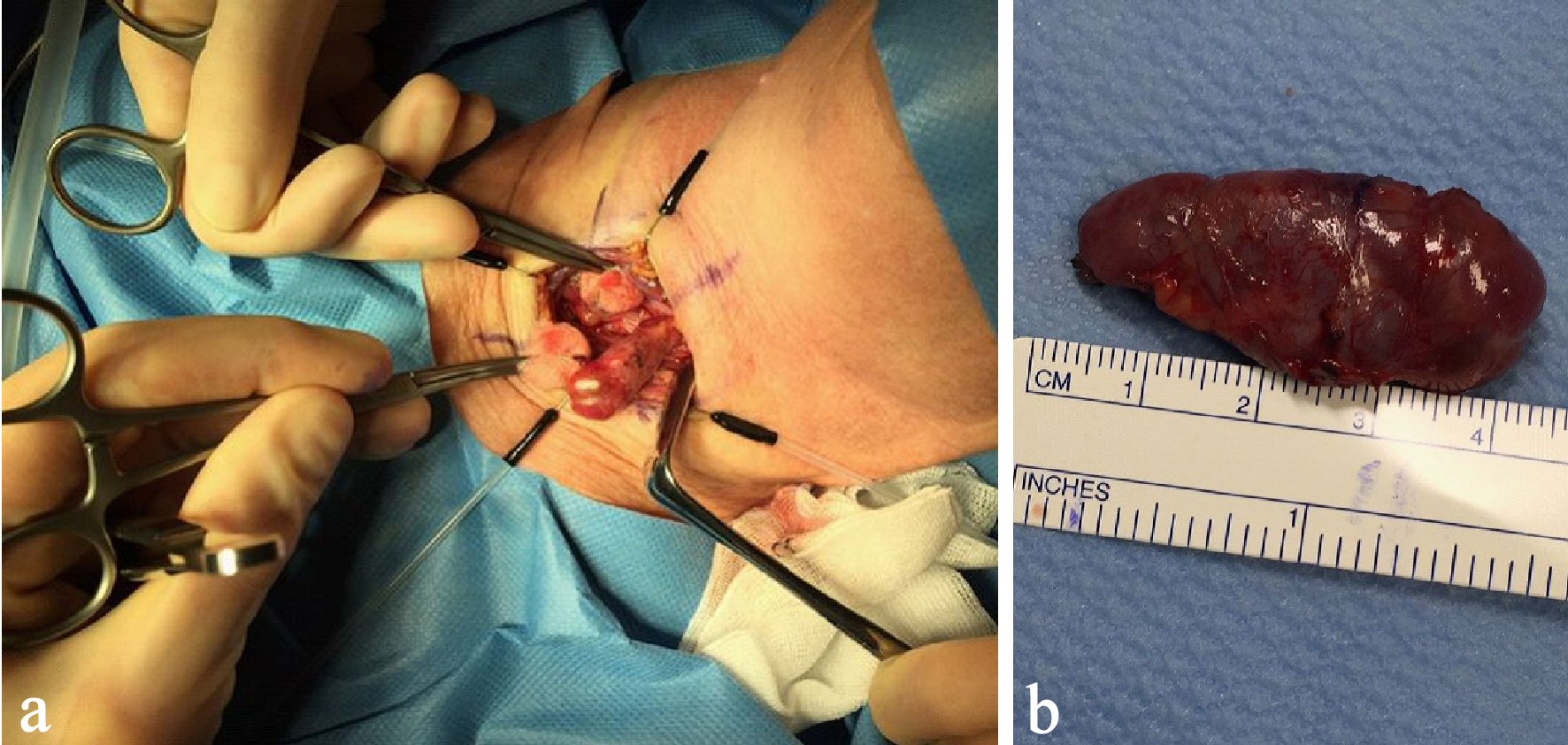
Figure 5. Per-operative image of the PTA (a) and postoperative image showing the adenoma of 4.9 g (b). PTA: parathyroid adenoma.
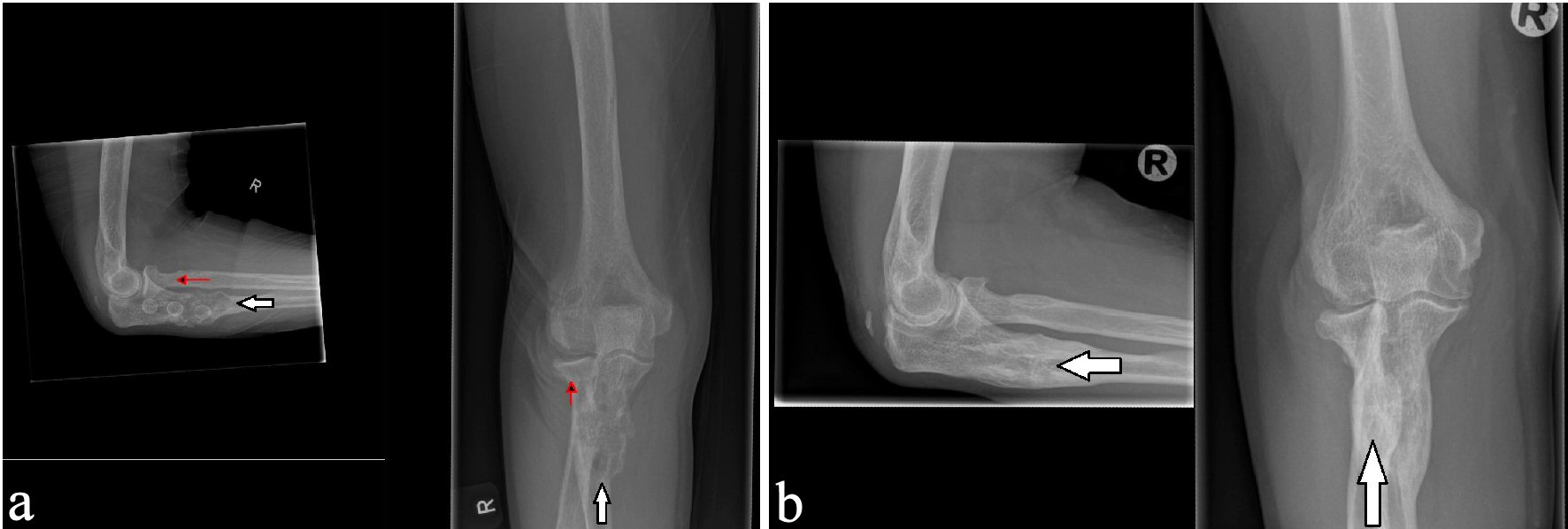
Figure 6. X-ray examinations after the fall trauma (a) and 14 months afterwards (b) showing regression of the osteolytic lesion in the ulna.
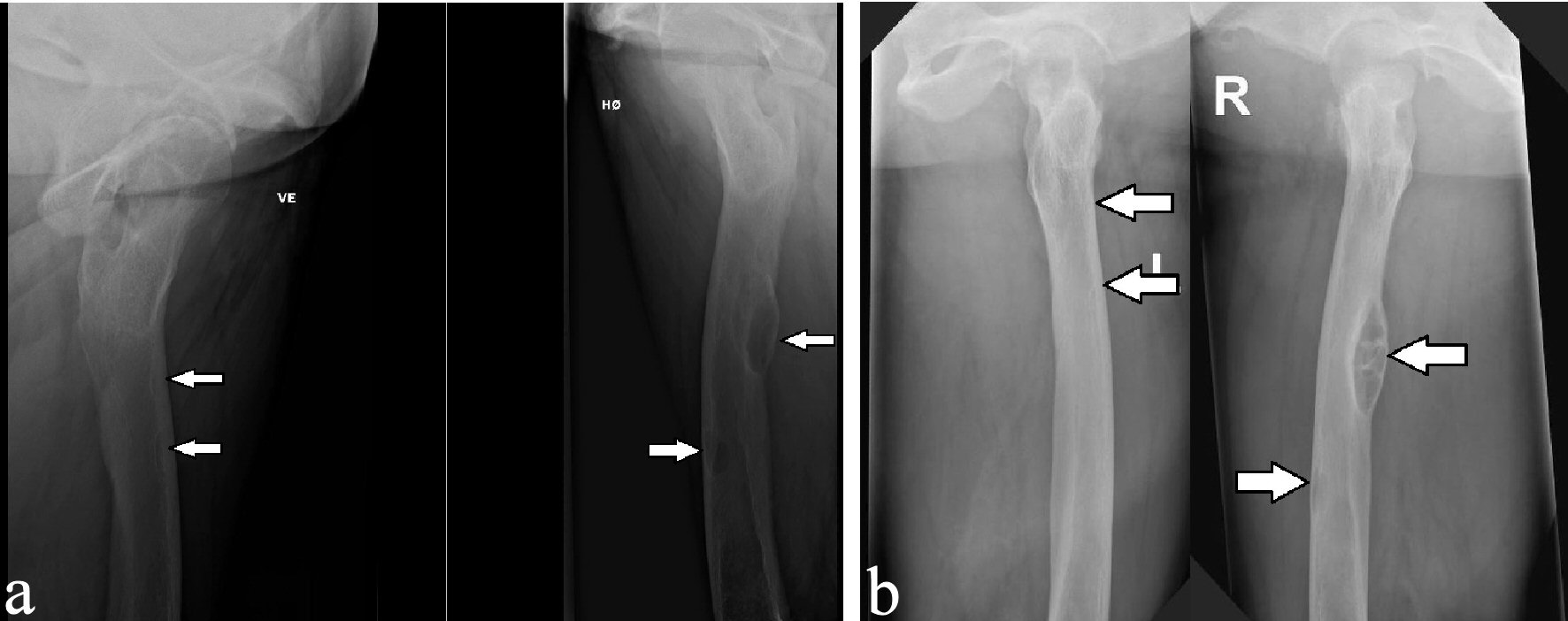
Figure 7. X-ray examinations after the fall trauma (a) and 14 months afterwards (b) showing regression of the osteolytic lesions in both femurs.
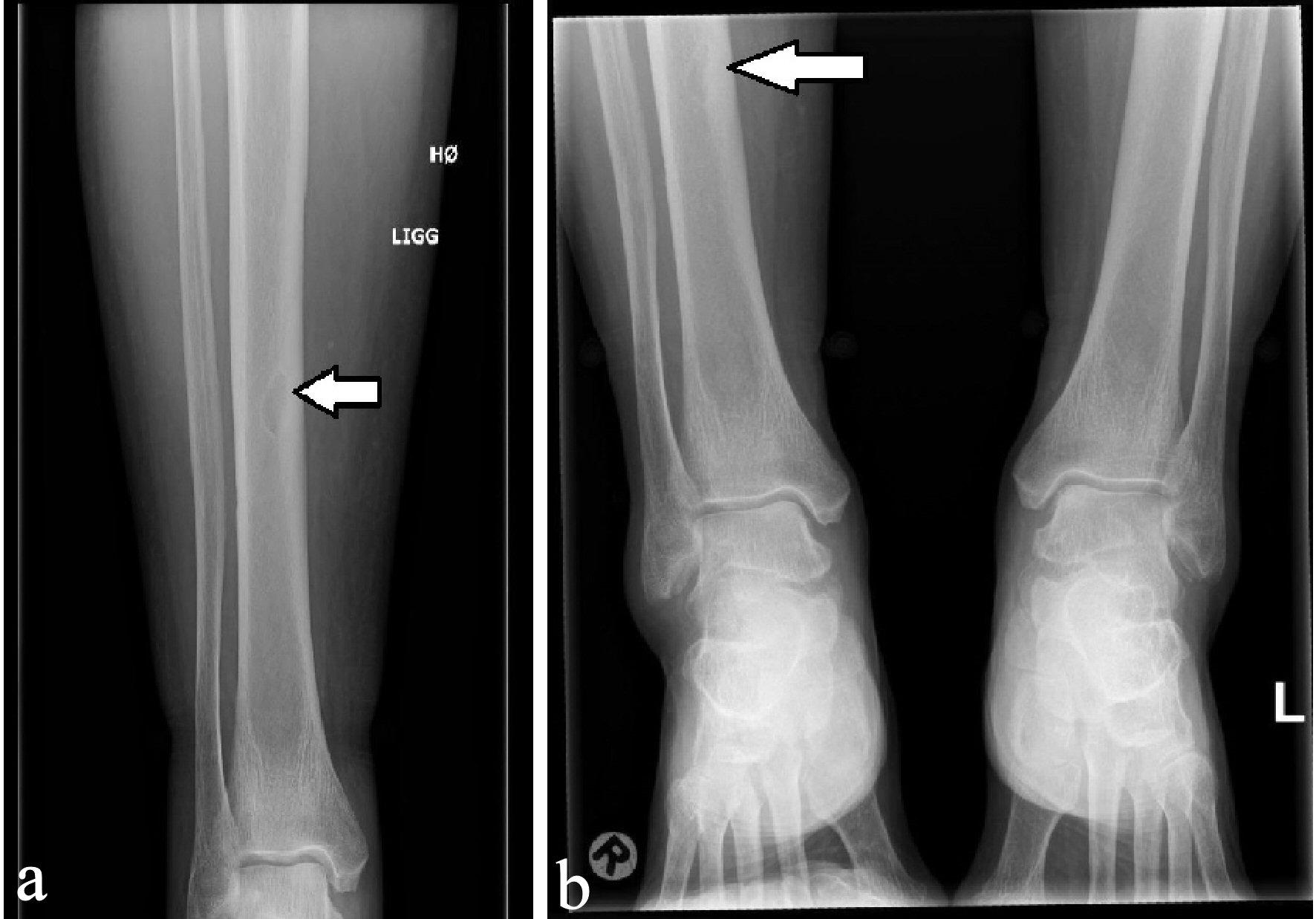
Figure 8. X-ray examinations after the fall trauma (a) and 14 months afterwards (b) showing regression of the osteolytic lesion in the tibia.