

| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website http://www.jofem.org |
Letter to the Editor
Volume 7, Number 2, April 2017, pages 72-74
Understanding of Dose-Response of Metformin by Using Continuous Glucose Monitoring
Taro Akiyamaa, b, Hidetaka Hamasakia, b, Hiroki Adachia, Hidekatsu Yanaia, c
aDepartment of Internal Medicine, National Center for Global Health and Medicine Kohnodai Hospital, Chiba, Japan
bThese authors equally contributed to this work.
cCorresponding Author: Hidekatsu Yanai, Department of Internal Medicine, National Center for Global Health and Medicine Kohnodai Hospital, 1-7-1 Kohnodai, Ichikawa, Chiba 272-0034, Japan
Manuscript accepted for publication April 25, 2017
Short title: Letter to the Editor
doi: https://doi.org/10.14740/jem419w
| To the Editor | ▴Top |
Metformin is widely used for the treatment of type 2 diabetes; however, the underlying mechanisms for blood glucose-lowering remain not fully understood. Metformin is known to reduce hepatic gluconeogenesis which is considered to be the main mechanism of glucose-lowering of metformin [1]. Metformin has been also reported to increase intestinal glucose utilization and reduce food intake, inducing weight reduction and resulting amelioration of insulin resistance [2, 3]. The activation of AMP-activated protein kinase (AMPK) which is a major cellular regulator of glucose metabolism was reported to be a main mechanism for metformin-mediated beneficial effects on diabetes [4], which was challenged by a recent report [5]. Then, metformin has been suggested to improve glucose metabolism by AMPK-dependent and AMPK-independent mechanisms [6].
Intravenous administration of metformin has been shown to be ineffective [7], and metformin was shown to increase plasma glucagon-like peptide-1 (GLP-1) [8].
Although the mechanisms for metformin-mediated increments in GLP-1 levels remain unknown, it has been hypothesized that metformin stimulates GLP-1 secretion directly and/or indirectly and prolongs the half-life of GLP-1, and that metformin may potentiate the glucose-lowering effects of GLP-1 by increasing target tissue sensitivity to GLP-1 [9]. Furthermore, metformin has been reported to suppress hepatic glucagon signaling by decreasing production of cyclic AMP [10].
Although various mechanisms have been suggested as metformin-mediated glucose-lowering, it remains unknown which of these mechanisms plays a crucial role at various daily doses of metformin. We performed a continuous glucose monitoring (CGM) in a 47-year-old type 2 diabetic male patient (body height, 171 cm; body weight, 77 kg; BMI, 26.3 kg/m2), referred to our hospital due to poor glucose control. He has been treated by using metformin (500 mg/day), linagliptin (5 mg/day) and empagliflozin (10 mg/day) for 3 weeks before admission at our outpatient clinic. His HbA1c level was 8.5% on admission. The treatment for his diabetes was shown in Figure 1.
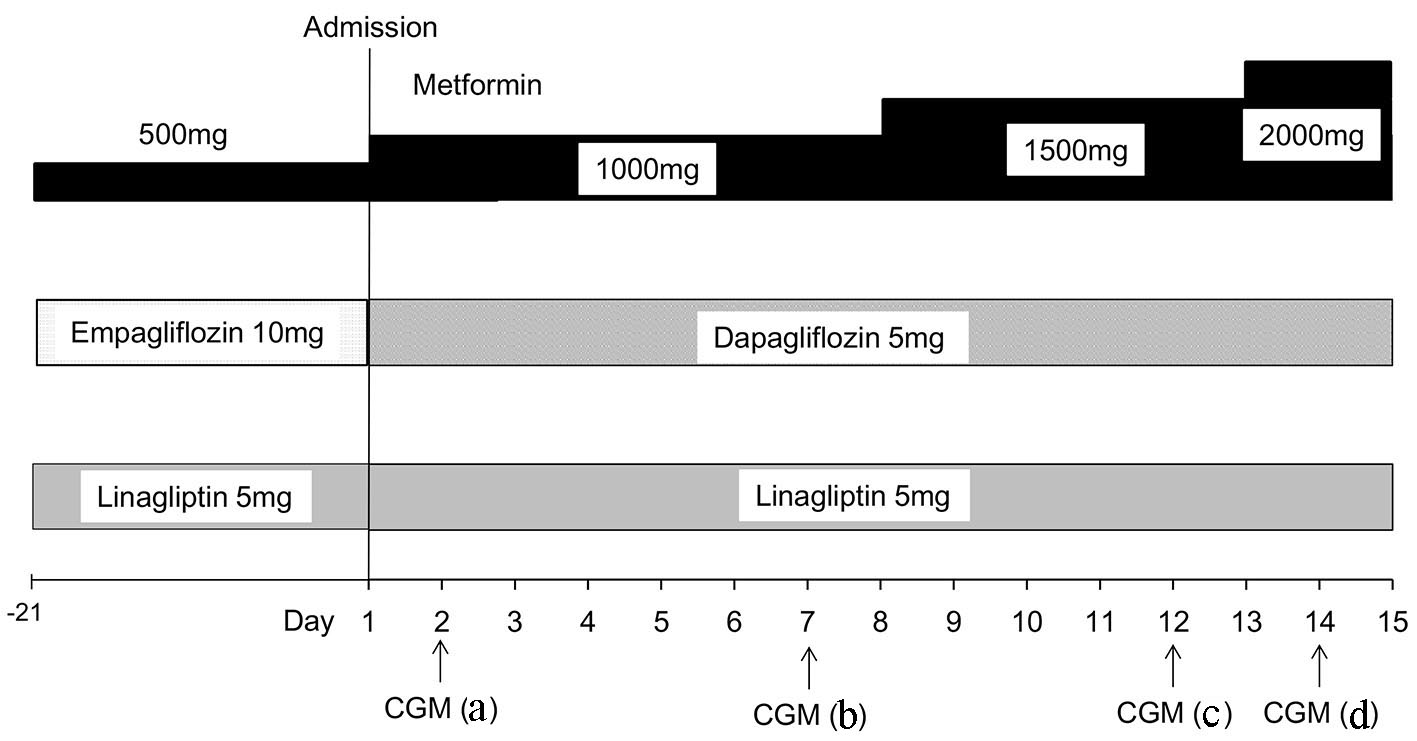 Click for large image | Figure 1. Treatment for type 2 diabetes before and after admission. Continuous glucose monitoring (CGM) a-d correspond with a-d in Figure 2. |
Results of CGM were shown in Figure 2. CGM showed hyperglycemia late at night and early at morning, suggesting that daily 500 - 1000 mg of metformin did not induce a sufficient suppression of hepatic gluconeogenesis and/or hepatic glucagon signaling. Daily 1,500 mg of metformin improved hyperglycemia late at night and early at morning, daily 1,500 mg may be needed to suppress hepatic gluconeogenesis and/or glucagon signaling. However, daily 1,500 mg of metformin could not suppress postprandial hyperglycemia, which was improved by daily 2,000 mg of metformin, indicating that daily 2,000 mg may be needed for an increment of GLP-1 secretion and/or activity.
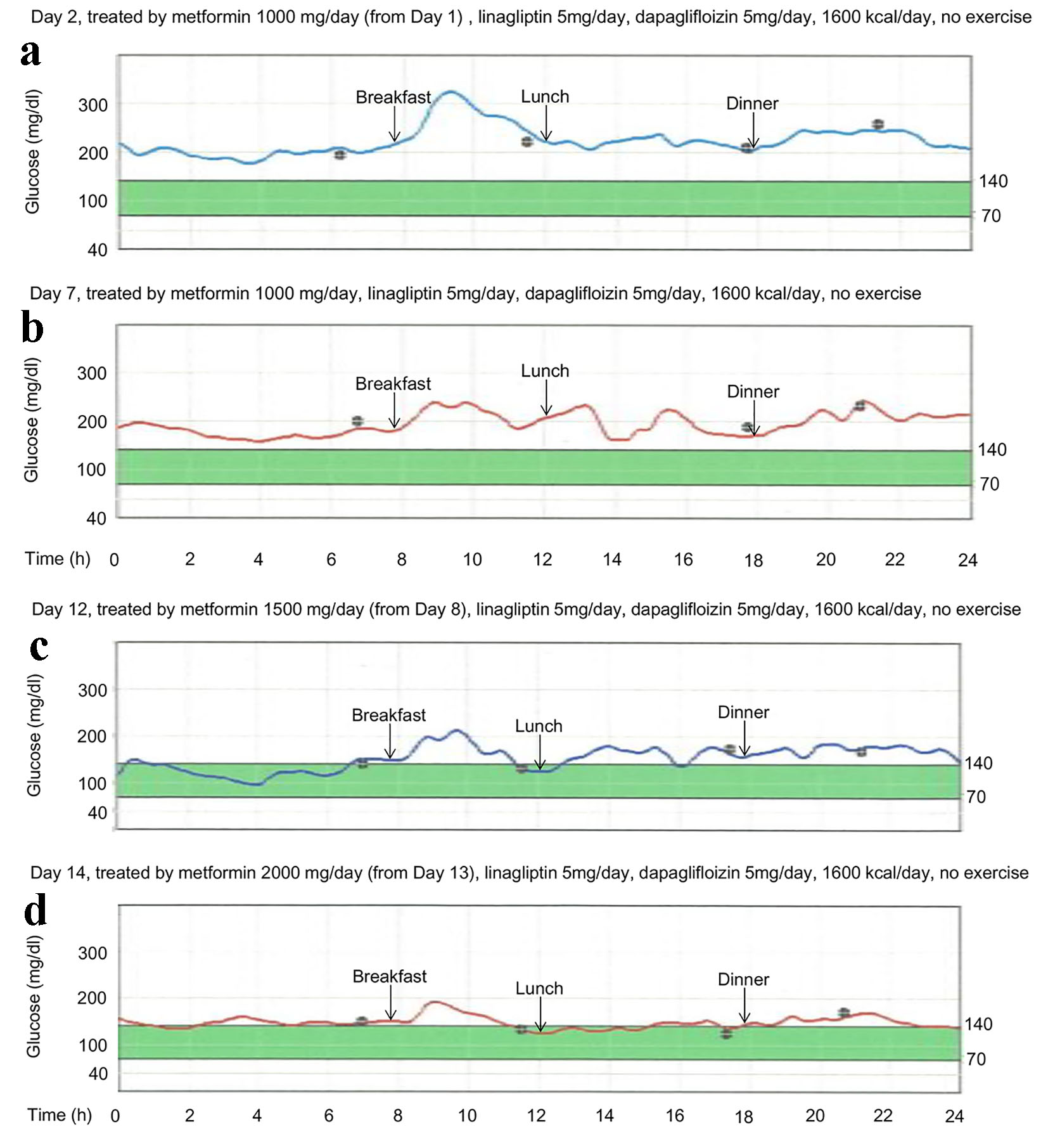 Click for large image | Figure 2. Continuous glucose monitoring (CGM) showing dose-response of metformin. |
We have to mention the limitation of our observation. First, this report is the observation of only one case. Second, other hypoglycemic agents may have an influence on the study results.
In conclusion, our observation of dose-response of metformin by using CGM may propose the glucose-lowering mechanism due to metformin varies depending on the dose.
Conflicts of Interests
The authors declare that they have no conflicts of interest concerning this article.
| References | ▴Top |
- DeFronzo RA, Barzilai N, Simonson DC. Mechanism of metformin action in obese and lean noninsulin-dependent diabetic subjects. J Clin Endocrinol Metab. 1991;73(6):1294-1301.
doi pubmed - Penicaud L, Hitier Y, Ferre P, Girard J. Hypoglycaemic effect of metformin in genetically obese (fa/fa) rats results from an increased utilization of blood glucose by intestine. Biochem J. 1989;262(3):881-885.
doi pubmed - Lee A, Morley JE. Metformin decreases food consumption and induces weight loss in subjects with obesity with type II non-insulin-dependent diabetes. Obes Res. 1998;6(1):47-53.
doi pubmed - Zhou G, Myers R, Li Y, Chen Y, Shen X, Fenyk-Melody J, Wu M, et al. Role of AMP-activated protein kinase in mechanism of metformin action. J Clin Invest. 2001;108(8):1167-1174.
doi pubmed - Foretz M, Hebrard S, Leclerc J, Zarrinpashneh E, Soty M, Mithieux G, Sakamoto K, et al. Metformin inhibits hepatic gluconeogenesis in mice independently of the LKB1/AMPK pathway via a decrease in hepatic energy state. J Clin Invest. 2010;120(7):2355-2369.
doi pubmed - Foretz M, Guigas B, Bertrand L, Pollak M, Viollet B. Metformin: from mechanisms of action to therapies. Cell Metab. 2014;20(6):953-966.
doi pubmed - Sum CF, Webster JM, Johnson AB, Catalano C, Cooper BG, Taylor R. The effect of intravenous metformin on glucose metabolism during hyperglycaemia in type 2 diabetes. Diabet Med. 1992;9(1):61-65.
doi pubmed - Mannucci E, Tesi F, Bardini G, Ognibene A, Petracca MG, Ciani S, Pezzatini A, et al. Effects of metformin on glucagon-like peptide-1 levels in obese patients with and without Type 2 diabetes. Diabetes Nutr Metab. 2004;17(6):336-342.
pubmed - Bahne E, Hansen M, Bronden A, Sonne DP, Vilsboll T, Knop FK. Involvement of glucagon-like peptide-1 in the glucose-lowering effect of metformin. Diabetes Obes Metab. 2016;18(10):955-961.
doi pubmed - Miller RA, Chu Q, Xie J, Foretz M, Viollet B, Birnbaum MJ. Biguanides suppress hepatic glucagon signalling by decreasing production of cyclic AMP. Nature. 2013;494(7436):256-260.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.